When exploring suicide data, it is important to remember that behind the numbers are people, families and communities impacted by suicide in Australia. The reasons people take their own life are complex, and often there is no single reason why a person attempts or dies by suicide. By increasing our understanding of data alongside the lived experience of distress, we will increase the opportunity to save lives.
For guidance on reporting on suicide and self-harm data, please refer to the Mindframe Quick Reference Guide.
Released by AIHW on Wednesday, 22 November 2023
- Culturally and Linguistically Diverse Australians: Suicide among refugee and humanitarian entrants and other permanent migrants
- LGBTIQ+ Australians: suicidal thoughts and behaviours and self-harm – Update to include Writing Themselves in 4 data
- Australian Defence Force suicide monitoring – annual update
- Suicide and self-harm monitoring factsheets and key messages
Culturally and Linguistically Diverse Australians: Suicide among refugee and humanitarian entrants and other permanent migrants
This update to the National Suicide and Self-harm Monitoring System includes a new page focused on suicide among refugee and humanitarian entrants and other permanent migrants. These data are drawn from a broader AIHW project investigating the health and welfare of Australia’s refugee and humanitarian entrant populations. The analysis uses a linked dataset that includes the Settlement Database from the Department of Home Affairs and the Australian Bureau of Statistics (ABS) Causes of Death dataset.
This update provides some insight into suicide among culturally and linguistically diverse (CALD) Australians. CALD communities and refugees are identified as priority populations in the National Mental Health and Suicide Prevention Agreement. Refugee and humanitarian entrants and other permanent migrant Australians included in this analysis are part of the broader CALD community in Australia. However these data are limited to those who have moved to Australia from another country (first-generation migrants) and should not be considered representative of broader CALD communities.
Specific variables included in this analysis are migration status (grouped as ‘Humanitarian entrants’, ‘Other permanent migrants’ and ‘Rest of the Australian Population’) and time since arrival (grouped as <5 years, 5-10 years, and >10 years). Deaths by suicide between 2007 and 2020 were examined.
Key findings:
First generation humanitarian entrants and other permanent migrants experienced lower rates of suicide compared to the rest of the Australian population.
- The age-standardised suicide rate for humanitarian entrants (6.7 per 100,000) and other permanent migrants (4.0 per 100,000) was lower than for the rest of the Australian population (12.6 per 100,000).
- Deaths by suicide were higher for males than females across all three migrant groups (see graph below). The largest difference was among humanitarian entrants, with the rate for males (11 per 100,000) being more than 3.5 times higher than for females (3.0 per 100,000). Among the rest of the Australian population, the rate for males was approximately three times higher than for females.
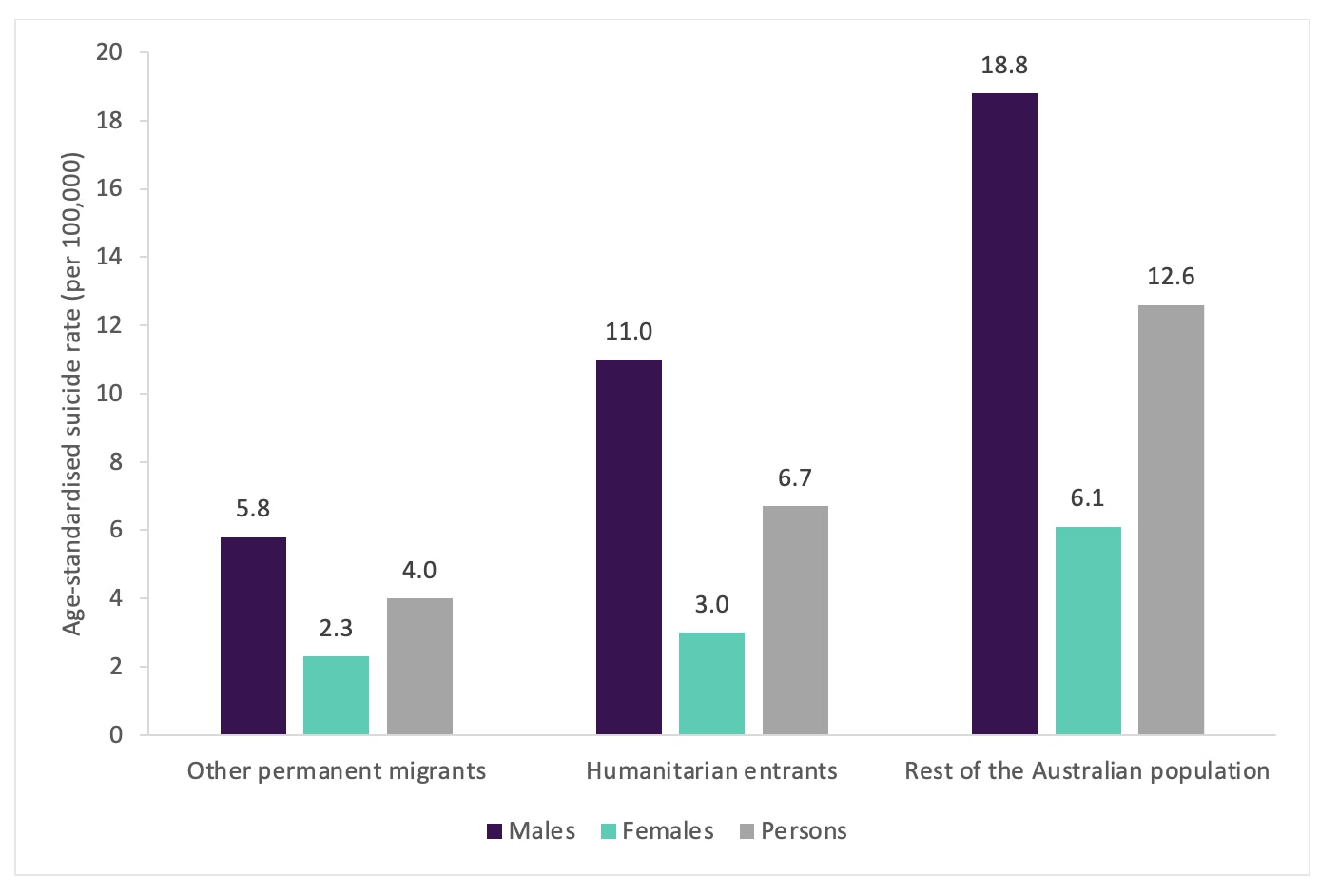
Adapted from AIHW’s Deaths by suicide by sex and migration group arriving on or after 2000, 2007-2020 viz
Rates of death by suicide for first generation humanitarian entrants and other permanent migrants increased with time since arriving in Australia
- Deaths by suicide increased for both humanitarian entrants and other permanent migrants as time since arrival in Australia increased.
- Humanitarian entrants had higher suicide rates compared to other permanent migrants at each period since arrival. However, when taking into account the error bars, the differences between these groups are small.
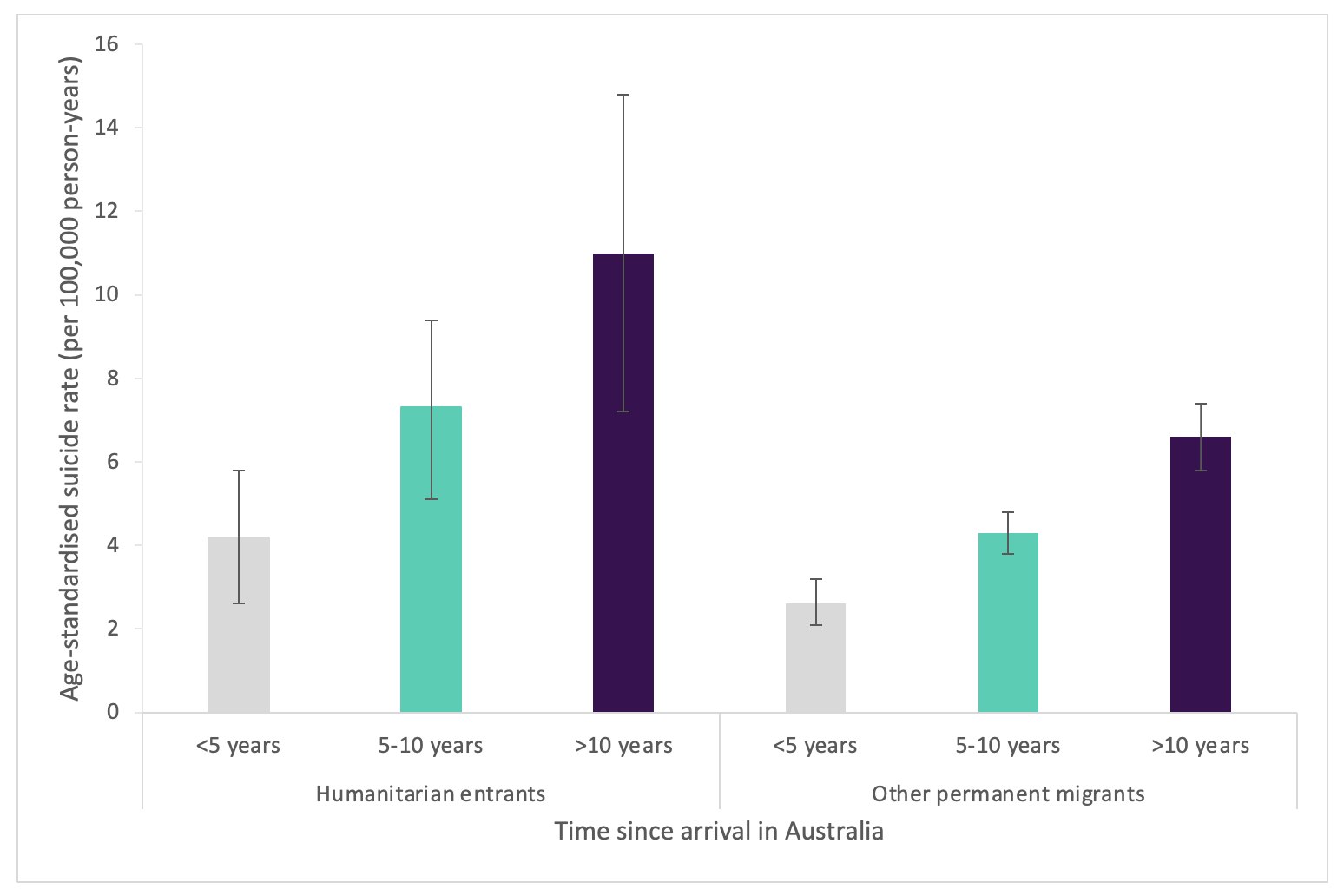
Reproduced from AIHW’s Deaths by suicide by time since arrival and migration group, 2007 – 2020 viz.
LGBTIQ+ Australians: suicidal thoughts and behaviours and self-harm
The National Suicide and Self-harm Monitoring System (the System) has been updated to include data from the Writing Themselves In 4 (WTI4) survey of lesbian, gay, bisexual, trans, intersex, queer, asexual and other sexuality, gender and bodily diverse (LGBTIQ+) young people.
People who identify as LGBTIQ+ are identified as a priority population for suicide prevention. However, there is currently no reliable national data on rates of suicide and self-harm among LGBTIQ+ communities in Australia. Without reliable data, it is difficult to estimate the extent of which LGBTIQ+ individuals are impacted by suicide and self-harm.
The best estimates of suicide and self-harm amongst the LGBTIQ+ individuals come from surveys that have specifically targeted LGBTIQ+ communities. These surveys often use non-probability sampling, meaning the data may not be representative of all LGBTIQ+ Australians. Despite this limitation, surveys still provide valuable information that can inform Australian suicide prevention efforts.
Private Lives 3 (PL3) and Writing Themselves In 4 (WTI4) are the largest and most comprehensive datasets available for LGBTQ+ Australians:
- PL3 sampled 6,835 LGBTQA+ adults aged between 18 and 88 years.
- WTI4 sampled 6,418 LGBTQA+ young people aged between 14 and 21 years.
Whilst PL3 and WTI4 attempted to recruit people with an intersex variation(s), the sample size was too small to make statistically meaningful comparisons. However, PL3 national report presents data from the 47 participants in a dedicated chapter (p. 93).
LGBTQ+ Adults (PL3)
These data were updated in the System on 7 July 2023, and a full summary is available here.
Key findings
- Around three-quarters (75%) of participants had experienced suicidal thoughts in their lifetime.
- Around one third (30%) of participants reported having attempted suicide in their lifetime.
- The prevalence of suicidal thoughts and attempts were similar across states and territories.
- Younger age groups were more likely to report lifetime or recent experiences of suicidal thoughts and suicide attempts compared to older age groups.
- The prevalence of suicidal thoughts and suicide attempts varied by sexual orientation. Pansexual and queer respondents reported the highest prevalence of recent and lifetime suicidal thoughts and lifetime suicide attempts.
- Trans and non-binary participants were more likely to have experienced recent and lifetime suicidal thoughts and suicide attempts compared to cisgender men and women.
- PL3 participants with a disability were more likely to report lifetime or recent experiences of suicidal thoughts and attempts than those without a disability.
LGBTQ+ young people (WTI4)
The Writing Themselves In 4 (WTI4) survey included questions on recent (last 12 months) and lifetime suicidal thoughts, self-harm, suicide plans and suicide attempts.
Use the below interactive map to filter specific data related to LGBTQA+ young people who experienced suicide thoughts, plans, attempts or self-harm over the last 12 months or ever.
The prevalence of suicidal thoughts, behaviours and self-harm were similar across sexual orientations. Pansexual, queer, and lesbian participants often had the highest percentage of suicidal and self-harming behaviour, whilst gay participants consistently had the lowest.
- Suicidal thoughts: Pansexual (85%), queer (83%), lesbian (82%), bisexual (79%) and participants classified as ‘something else’ (79%) reported the highest lifetime prevalence for suicidal thoughts, followed by asexual (75%) and gay (69%) participants. A similar pattern was seen for recent suicidal thoughts.
- Suicide plans: Pansexual participants had the highest rates of lifetime (57%) and recent (31%) suicide plans, while gay participants had the lowest (38% and 18%, respectively).
- Suicide attempts: 35% of pansexual participants, 30% of lesbian participants, 30% of queer participants, 26% of participants classified as ‘something else’, 24% of bisexual participants, 21% of asexual participants, and 19% of gay participants had attempted suicide in their lifetime. For recent suicide attempts, lesbian participants (14%) had the highest percentage, followed by pansexual (13%) and queer participants (12%).
- Self-harm: Both lifetime and recent self-harm followed a similar pattern to suicidal thoughts and plans.
Trans men, trans women and non-binary participants were more likely to have experienced lifetime or recent self-harm, suicide attempt, thoughts of suicide or have made a suicide plan, compared to cisgender men and women.
- Trans men had higher lifetime prevalence of suicidal thoughts (92%) and suicide attempts (47%) compared to trans women (91% and 40%, respectively).
- Trans women had higher prevalence of recent suicidal thoughts (77%) and suicide attempts (20%), compared to trans men (73% and 17%, respectively).
There was little difference in prevalence of lifetime or recent suicidal thoughts, suicide plans, suicide attempts and self-harm behaviours by state or territory.
- Suicidal thoughts: Participants from Tasmania (86%) or the Northern Territory (84%) were more likely to experience lifetime suicidal thoughts.
- Suicide plans: The percentage of participants who had made a plan to attempt suicide in their lifetime ranged from 45% in Victoria to 54% in Tasmania. Tasmania also had the highest proportion of participants who had recently (in the last 12 months) planned to take their own life (30%).
- Suicide attempts: The proportion of participants who had attempted suicide in their lifetime ranged from 23% in the Northern Territory to 30% in Tasmania. However, Northern Territory participants had the highest proportion of recent (in the last 12 months) suicide attempts (15%).
Lifetime prevalence of suicidal thoughts, suicide attempts, and self-harm were similar between the 14-17 year and the 18–21 year age group across sexual orientation categories.
- Recent (in the last 12 months) suicide attempts and self-harm were more common in participants in the 14-17 year age group compared to the 18-21 year age group across all sexual orientations, except asexuality.
- Recent (in the last 12 months) suicidal thoughts were more common amongst 14–17 year olds compared to 18–21 year olds across all sexual orientations, except bisexuality. Though, these differences were small.
Among gender classifications there was little difference between participants aged 14 to 17 years and 18 to 21 years in reported lifetime suicidal thoughts, suicide attempt, and self-harm except for trans women.
- Trans women aged 14 to 17 years (27%) were about half as likely as those aged 18 to 21 years (50%) to experience lifetime suicide attempt and lifetime self-harm (49% and 83%, respectively).
- Almost all genders reported a higher likelihood of recent suicidal thoughts, suicide attempt and self-harm in the 14 to 17 years age group, compared to the 18 to 21 years age group. However, trans women aged 14 to 17 years (15%) were less likely than those aged 18 to 21 years (24%) to experience recent suicide attempt, and about half as likely to experience recent self-harm (33% and 60%, respectively).
Note: Results for trans women should be interpreted with caution due to low numbers in the survey.
Support service use
- Sexual orientation: Pansexual (62%), queer (59%) and participants and those classified as ‘something else’ (54%) were most likely to access professional support services in relation to suicide or self-harm, followed by lesbian (53%), bisexual (50%), asexual (47%) and gay participants (41%).
- Gender: Trans men (71%), trans women (64%), non-binary (57%), and cisgender women (51%) were more likely to report having accessed professional support services, followed by cisgender men (39%).
- Disability: Participants with a disability (69%) were more likely to access professional support service in relation to suicide or self-harm, than participants without a disability (39%).
- State or territory: Participants in the Australian Capital Territory (65%) were more likely to access professional support services in relation to suicide or self-harm, with participants from the Northern Territory (42%) the least likely. However, access to professional telephone support services was highest in the Northern Territory (17%), with participants from Queensland being least likely (9%).
Australian Defence Force Suicide Monitoring – annual update
The Australian Defence Force suicide monitoring page of the Suicide and Self-harm Monitoring site has been updated with data from the Serving and ex-serving Australian Defence Force members who have served since 1985: suicide monitoring 1997 to 2021 report (released 21 November 2023). Life in Mind provides a translation of this report here.
Suicide and self-harm monitoring factsheets and key messages
Everymind, in partnership with AIHW, has developed resources to support understanding and use of data in the National Suicide and Self-harm Monitoring System, and guide responsible reporting. These include:
- Factsheet - What is the National Suicide and Self-harm Monitoring System
- Factsheet - Statistical terms explained
- Factsheet - Understanding geographic data in the National Suicide and Self-harm Monitoring System
- Factsheet - Understanding hospitalisation and ambulance data in the National Suicide and Self-harm Monitoring System
- Mindframe Quick reference guide for communicating safely about suicide and self-harm data
- Infographic snapshots of suicide data across multiple population groups reflecting the data presented in the National Suicide and Self-harm Monitoring System.
These are available for download on the Life in Mind portal, as well as through the Suicide and Self-harm Monitoring System.